
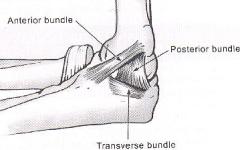
The medial collateral ligament (MCL) of the elbow is critical for valgus stability of the elbow and is the primary elbow stabilizer.
As such, the MCL plays an important role in most throwing sports, including baseball and javelin, as well as racquet sports and ice hockey. Elbow injuries in young athletes generally are chronic, with persistent pain and instability from repetitive overhead activities. In the athlete, ligamentous injury can also be heralded by an acute traumatic event such as an elbow dislocation. This can lead to chronic pain and valgus instability.
Medial elbow pain in athletes who throw is the most common symptom. Pain may be especially prominent during the acceleration phase of the overhead throw. Pain is often chronic or recurrent and may lead to a slow erosion of throwing ability. Athletes may report similar pain in previous seasons. Rest generally helps relieve pain. Occasionally, athletes may experience acute pain over the medial elbow, sometimes associated with a popping sensation, during a single throw that causes them to stop throwing immediately.
Medial elbow tenderness and swelling are the most notable findings. MCL tenderness may occasionally be difficult to differentiate from flexor pronator tendonitis, but the pain of flexor pronator tendinitis is aggravated by resisting forearm pronation. Loss of elbow range of motion (ROM) is occasionally observed. With acute rupture, ecchymosis may be observed over the medial elbow. Pain may be reproduced on making a clenched fist. Valgus stress with the elbow in 25° of flexion (elbow abduction stress test) reproduces pain and may cause joint opening. The affected side should be compared with the contralateral elbow as a reference for baseline laxity. MRI may confirm ligement tear or partial tear. Plain x-ray may show calcification, osteochondritis dessicans, or posteromedial spurring from valgys overload related impingement. This plain film shows calcification at the MCL origin. 
A complete tear was present, and intraoperative valgus stress revealed pathologic joint opening.

Surgical Intervention
Direct repair of the ligament is not generally indicated. Reconstruction of the MCL is the more common approach to surgical treatment using a palmaris longus tendon autograft. Repair of the anterior bundle of the UCL is undertaken with a palmaris longus tendon graft or with allograft.
The graft can be secured via bone tunnels, a so-called "docking technique", hybrid techniques, or tenodesis screws at the sublime tubercle and within the medial epicondyle, as was performed in this case.


Physical Therapy
After surgery, the elbow is immobilized in a posterior splint for 10 days in 90° of flexion. Active ROM is initiated after removal of the posterior splint. A hinged brace that prevents valgus stress should be used. At approximately 1 month after surgery, isometric strengthening exercises should be initiated. Limited progressive strengthening can be initiated at 8 weeks and plyometrics at 12 weeks. Shoulder and elbow exercises should be instituted as soon as feasible, but valgus stress of the elbow should be avoided for at least 4-6 months until the graft has had sufficient time to incorporate. After 4-6 months, throwing may be resumed with a training program designed to return to competitive throwing no sooner than 9-12 months after surgery.
Outcomes
Literature review shows outcomes in the mid 80% range, and retear rate can range between 1 and 5%. The average "pitching" career length following reconstruction for major league pitchers is about 4 years based on the literature. Dr. James Andrews large series showed an 80% return to baseball, but only 75% made it back to the major leagues.In short, this procedure may "reset the bell" for a period of time, but is not likely to provide an indefinite, permanent solution. It is imperative, therefore, to prevent such injury in the first place by adhering to pitching limits, ensuring proper mechanics and core strength.

